
ooeat0meoo
Member of the Muppet Empire
I need help with how other countries outside the USA are dealing with the opioid epidemic and other addictions.
Over the past 5 months, I've been doing research on mental health and substance use disorder, with a primary focus on the increasing overdose rates throughout New York State. The trend for legislative and government policy and funding over the past 5+ years has been Harm Reduction. The pharmaceutical solution in NY State and throughout most of the United States has been Suboxone Buprenorphine/Naloxone, being the preferred choice over the traditionally more addictive Methadone according to the Substance Abuse and Mental Health Services Administration (SAMHSA) national agency. Under this umbrella term of 'Harm Reduction' are two other elements of attack, Narcan training and distribution and peer advocacy. Narcan is a nose spray that reverses an opioid overdose. Peer advocates are very much like 12 Step program sponsors, only peer advocates go through a year of training before becoming certified to help new people in recovery on their own.
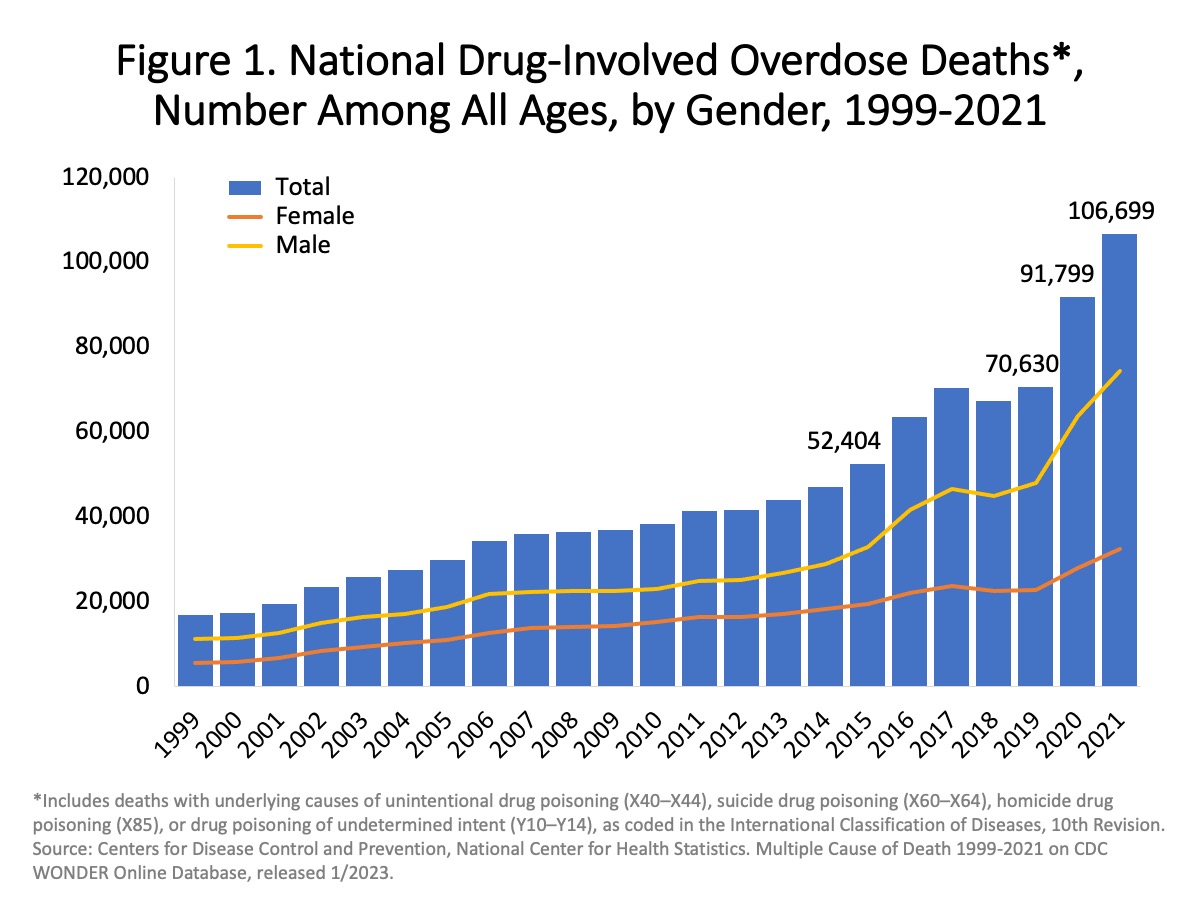
As you can see here on this graph, opioid fatalities have increased by more than 100% since 2015 in the USA. A significant reason, as most of us know by now is due to the increase of Fentanyl and now traffickers are mixing in an animal tranquilizer Xylazine (Tranq) to extend the effects of heroin and Fentanyl. This development has had a massive impact on the death rates. According to a report by Vice News recently, more than 90% of the supply on heroin and Fentanyl in the Philadelphia area has traces of Xylazine, now.
As I said, I've been looking into this for more than 5 months. It's been an interesting ride because my understanding of how people with addictions were treated is they'd go to a detox and then a treatment facility, then transition to a halfway house, and then back into life on their own. I'm utterly shocked by what I'm finding out about the prevailing environment of recovery services in the US. Post Acute Withdrawal Syndrome (PAWS) characterizes the damage of an addict's brain by being numbed by alcohol and drug usage. It is proven to take 6 months to 2 years for the brain to recalibrate, in addition it usually takes 7 years of complete abstinence for one to get completely back on track with maturity development. The science of this reality is now suppressed and ignored.
If you've seen the movie Idiocracy, that's a perfect analogy of our response to the opioid epidemic in America. I've interviewed politicians (local/state/federal), addiction agency leaders, service providers, and coalition leaders. Very few of these involved want to return to funding inpatient treatment. Some don't expect to attract educated drug and alcohol councilors/therapists to work with this population as it's been seen as unaffordable. At the moment there's $2 billion set aside from settlements with opioid pharmaceutical companies like Perdue (Sacklers), ready to be distributed, but so many politicians are used to doing nothing, so nothing is being done, so far.
Everyone involved has been sticking with the low budget band-aid solution of medicating opioid users and flooding the system with peer advocates (remember PAWS which implies their brains are still a bit scrambled), and then... I spoke with a leader in the field of recovery who told me a few days ago, that he knows of 4 peer advocates that are all getting high and/or drinking alcohol. One peer advocate actually smokes weed with all of his clients. In addition, there is no expectation of complete abstinence from peer advocates.
What I need to know...
Is this the same sort of thing happening in other countries?
Over the past 5 months, I've been doing research on mental health and substance use disorder, with a primary focus on the increasing overdose rates throughout New York State. The trend for legislative and government policy and funding over the past 5+ years has been Harm Reduction. The pharmaceutical solution in NY State and throughout most of the United States has been Suboxone Buprenorphine/Naloxone, being the preferred choice over the traditionally more addictive Methadone according to the Substance Abuse and Mental Health Services Administration (SAMHSA) national agency. Under this umbrella term of 'Harm Reduction' are two other elements of attack, Narcan training and distribution and peer advocacy. Narcan is a nose spray that reverses an opioid overdose. Peer advocates are very much like 12 Step program sponsors, only peer advocates go through a year of training before becoming certified to help new people in recovery on their own.
As you can see here on this graph, opioid fatalities have increased by more than 100% since 2015 in the USA. A significant reason, as most of us know by now is due to the increase of Fentanyl and now traffickers are mixing in an animal tranquilizer Xylazine (Tranq) to extend the effects of heroin and Fentanyl. This development has had a massive impact on the death rates. According to a report by Vice News recently, more than 90% of the supply on heroin and Fentanyl in the Philadelphia area has traces of Xylazine, now.
As I said, I've been looking into this for more than 5 months. It's been an interesting ride because my understanding of how people with addictions were treated is they'd go to a detox and then a treatment facility, then transition to a halfway house, and then back into life on their own. I'm utterly shocked by what I'm finding out about the prevailing environment of recovery services in the US. Post Acute Withdrawal Syndrome (PAWS) characterizes the damage of an addict's brain by being numbed by alcohol and drug usage. It is proven to take 6 months to 2 years for the brain to recalibrate, in addition it usually takes 7 years of complete abstinence for one to get completely back on track with maturity development. The science of this reality is now suppressed and ignored.
If you've seen the movie Idiocracy, that's a perfect analogy of our response to the opioid epidemic in America. I've interviewed politicians (local/state/federal), addiction agency leaders, service providers, and coalition leaders. Very few of these involved want to return to funding inpatient treatment. Some don't expect to attract educated drug and alcohol councilors/therapists to work with this population as it's been seen as unaffordable. At the moment there's $2 billion set aside from settlements with opioid pharmaceutical companies like Perdue (Sacklers), ready to be distributed, but so many politicians are used to doing nothing, so nothing is being done, so far.
Everyone involved has been sticking with the low budget band-aid solution of medicating opioid users and flooding the system with peer advocates (remember PAWS which implies their brains are still a bit scrambled), and then... I spoke with a leader in the field of recovery who told me a few days ago, that he knows of 4 peer advocates that are all getting high and/or drinking alcohol. One peer advocate actually smokes weed with all of his clients. In addition, there is no expectation of complete abstinence from peer advocates.
What I need to know...
Is this the same sort of thing happening in other countries?

") My last paragraph is overly dramatic and yours is spot on.
My last paragraph is overly dramatic and yours is spot on.