
For what is worth in my case during the onset of symptoms the antigen test that I did came back negative, after 2 days I went to do a PCR (since symptoms were not going away) which has detected virus.I get that PCRs are the best tests, I'm just wondering about the value of a test done on Tuesday for a flight on Friday.
From what I've read on infectiousness - people are reckoned to be at their most infectious +/- two days from symptoms onset. Hence the relative inaccuracy of the LFT (picking up about 50% of cases) in week two doesn't necessarily make it useless, especially as week one it's thought to be 70%
It's how to calculate that trade off between testing people on the day versus testing them too early that I'm curious about. I just wondered if anyone has seen some actual modelling on it, or is it just the broad principle of "PCR better" that makes the decision, despite the test being done at the wrong time.
SARS CoV-2 coronavirus / Covid-19 (No tin foil hat silliness please)
- Thread starter Don't Kill Bill
- Start date
Pogue Mahone
The caf's Camus.
I get that PCRs are the best tests, I'm just wondering about the value of a test done on Tuesday for a flight on Friday.
From what I've read on infectiousness - people are reckoned to be at their most infectious +/- two days from symptoms onset. Hence the relative inaccuracy of the LFT (picking up about 50% of cases) in week two doesn't necessarily make it useless, especially as week one it's thought to be 70%
It's how to calculate that trade off between testing people on the day versus testing them too early that I'm curious about. I just wondered if anyone has seen some actual modelling on it, or is it just the broad principle of "PCR better" that makes the decision, despite the test being done at the wrong time.
I think @F-Red is right. It’s a test within 72 hours you need, which gives a bit of wriggle room. If it was within 24-48 hours you could get people being sent home from their destination due to delays or stop-overs that take longer than planned.
On the day supervised LFT would also be useful but logistically much more complex if we’re asking people to do it at airports. The PCR is consistently accurate and it’s up to the traveller to arrange it at their own time/expense.
"The sensitivity of antibody-based rapid diagnostic testing increased with duration of illness, from 26.8% sensitivity (18.3-36.8) in week one to 76.4% (70.1-82.0) 14 days after symptom onset." https://doi.org/10.1016/S1473-3099(21)00152-3I get that PCRs are the best tests, I'm just wondering about the value of a test done on Tuesday for a flight on Friday.
From what I've read on infectiousness - people are reckoned to be at their most infectious +/- two days from symptoms onset. Hence the relative inaccuracy of the LFT (picking up about 50% of cases) in week two doesn't necessarily make it useless, especially as week one it's thought to be 70%
It's how to calculate that trade off between testing people on the day versus testing them too early that I'm curious about. I just wondered if anyone has seen some actual modelling on it, or is it just the broad principle of "PCR better" that makes the decision, despite the test being done at the wrong time.
Another analytical concern is that there are plenty of LFT kits in the market with varying performances. Some countries are using kits with very poor sensitivity. It is impossible to standardize and create a model for it on an international level.
That's the antibody test though - presumably a blood test - where you'd expect to have to wait for the antibodies to develop. The ones I was thinking about were the swab type antigen tests like the LFTs being used for rapid testing in the UK."The sensitivity of antibody-based rapid diagnostic testing increased with duration of illness, from 26.8% sensitivity (18.3-36.8) in week one to 76.4% (70.1-82.0) 14 days after symptom onset." https://doi.org/10.1016/S1473-3099(21)00152-3
Another analytical concern is that there are plenty of LFT kits in the market with varying performances. Some countries are using kits with very poor sensitivity. It is impossible to standardize and create a model for it on an international level.
From the same report:
Antigen-based rapid diagnostic test sensitivity was 80·0% (95% CI 71·0–88·0) in the first 7 days after symptom onset, but antibody-based rapid diagnostic tests had only 26·8% sensitivity (18·3–36·8).
It's noticeably weaker on asymptomatic cases, and the antigens fade as the antibodies rise - but it still feels like a useful "on the day" measure compared to a 3 day old test.
I think I'd feel safer with someone who tested (supervised) LFT antigen negative on the day sat next to me on the plane, rather than someone PCR negative three days ago - though obviously a "do both" or a "don't travel" plan is better. But if someone has fed the data into some kind of statistical model, I'd be intrigued to see it.
"Data on the sensitivity and specificity of currently available Ag-RDTs for SARS-CoV-2 have been derived from studies that vary in design and in the test brands being evaluated. They have shown that sensitivity compared to NAAT in samples from upper respiratory tract (nasal or nasopharyngeal swabs) appears to be highly variable, ranging from 0-94% but specificity is consistently reported to be high (>97%)." https://apps.who.int/iris/bitstream...HO-2019-nCoV-Antigen_Detection-2020.1-eng.pdfThat's the antibody test though - presumably a blood test - where you'd expect to have to wait for the antibodies to develop. The ones I was thinking about were the swab type antigen tests like the LFTs being used for rapid testing in the UK.
From the same report:
Antigen-based rapid diagnostic test sensitivity was 80·0% (95% CI 71·0–88·0) in the first 7 days after symptom onset, but antibody-based rapid diagnostic tests had only 26·8% sensitivity (18·3–36·8).
It's noticeably weaker on asymptomatic cases, and the antigens fade as the antibodies rise - but it still feels like a useful "on the day" measure compared to a 3 day old test.
I think I'd feel safer with someone who tested (supervised) LFT antigen negative on the day sat next to me on the plane, rather than someone PCR negative three days ago - though obviously a "do both" or a "don't travel" plan is better. But if someone has fed the data into some kind of statistical model, I'd be intrigued to see it.
I'm sorry for my mistake, yet the analytical issue on rapid antigen tests remains unsolved. I'd feel safe if all LFT kits have a sensitivity of 80%, but unfortunately plenty of kits do not offer such a high sensitivity and it's hard to tell which kit is adopted by other countries.
You've got a point about the three-day gap, but I think same-day LFTs can only act as an adjunct to the PCR.
72 hrs isn't much by the time you get the test results back.and travel.Surely the 3 days is to cover transit time as well? Especially for those travelling longer distances, my other half's relative had an issue where his PCR test had expired after a nightmare journey coming from the USA to the UK.
All a numbers game. Some people could test negative despite being infected because the viral loads was still building but still far better than the worst performance of the rapid tests (2nd week of infection). If you want to stop importing any covid you need a quarantine system as well.The issue is one I've struggled with too. There just seems to be a lot of time for things to happen in 72 hours, so much so that a 3 day old PCR rest may no longer be relevant even if it was negative at the time.
I think the PCR timeline is set by the sheer practicality of taking a test and getting a result in time to fly. It's just what that does to it's actual usefulness that I'm wondering about.72 hrs isn't much by the time you get the test results back.and travel.
From https://www.gov.uk/guidance/how-to-quarantine-when-you-arrive-in-england
"You must take the test in the 3 days before the service on which you will arrive in England departs. For example, if you travel directly to England on Friday, you must take the test on the Tuesday, Wednesday or Thursday."
Yes and there's nothing wrong with that.I think the PCR timeline is set by the sheer practicality of taking a test and getting a result in time to fly. It's just what that does to it's actual usefulness that I'm wondering about.
From https://www.gov.uk/guidance/how-to-quarantine-when-you-arrive-in-england
"You must take the test in the 3 days before the service on which you will arrive in England departs. For example, if you travel directly to England on Friday, you must take the test on the Tuesday, Wednesday or Thursday."
https://www.manchestereveningnews.co.uk/news/government-advises-against-travel-out-20667478
Well that's interesting.
Edit - it's changed, there was mention of recording motorway travel and fining in an earlier version.
Well that's interesting.
Edit - it's changed, there was mention of recording motorway travel and fining in an earlier version.
Rado_N
Yaaas Broncos!
Avoiding Bolton is always a good idea tbf.
Stanley Road
Renaissance Man
Is there ever a reason to visit Bolton?Avoiding Bolton is always a good idea tbf.
Rado_N
Yaaas Broncos!
I can’t think of one.Is there ever a reason to visit Bolton?
You don't visit Bolton, but you might have to go through it to get to the West Pennine Moors on the other side.
My sister and BIL recently had to leave their rented house in Bolton after living there for many years, and I did all the online searching for a new place for them (I have time on my hands). I found them a nice place in the countryside near Chorley. Bolton is grim, in my opinion.Avoiding Bolton is always a good idea tbf.
Classical Mechanic
Full Member
Lovely town hall and civic centre for a town of it's size.Is there ever a reason to visit Bolton?
And the car park for Bolton Screwfix is really good, spacious and well locatedLovely town hall and civic centre for a town of it's size.

I'm feeling pretty negative about the other shops there though.
Rado_N
Yaaas Broncos!
Nice, there’s some lovely areas around Chorley.My sister and BIL recently had to leave their rented house in Bolton after living there for many years, and I did all the online searching for a new place for them (I have time on my hands). I found them a nice place in the countryside near Chorley. Bolton is grim, in my opinion.
Gehrman
Phallic connoisseur, unlike shamans
- Joined
- Feb 20, 2019
- Messages
- 11,171
Is the lab-leak hypothesis considered a unsubstantiated conspiracy theory in this thread? It seems it's gaining more recognition as a possible origin at the moment.
https://www.washingtonpost.com/poli...han-lab-leak-theory-suddenly-became-credible/
https://www.washingtonpost.com/poli...han-lab-leak-theory-suddenly-became-credible/
Last edited:
Would love to review your sources on this?Is the lab-leak hypothesis considered a unsubstantiated conspiracy theory in this thread? It seems it's gaining more recognition as a possible origin at the moment.
Gehrman
Phallic connoisseur, unlike shamans
- Joined
- Feb 20, 2019
- Messages
- 11,171
I put a link above. It contains links to most of the articles of interest. Fauchi has also begun to doubt that the virus evolved naturally.Would love to review your sources on this?
https://nicholaswade.medium.com/origin-of-covid-following-the-clues-6f03564c038
prateik
Full Member
- Joined
- Dec 14, 2005
- Messages
- 42,183
where ?I put a link above. It contains links to most of the articles of interest. Fauchi has also begun to doubt that the virus evolved naturally.
https://nicholaswade.medium.com/origin-of-covid-following-the-clues-6f03564c038
Gehrman
Phallic connoisseur, unlike shamans
- Joined
- Feb 20, 2019
- Messages
- 11,171
prateik
Full Member
- Joined
- Dec 14, 2005
- Messages
- 42,183
thanks..
first I have heard anyone credible suggest it might not have evolved naturally.
Bosws87
Full Member
- Joined
- Jun 18, 2015
- Messages
- 3,729
Too sensible for humans as a whole, but surely you would of developed some form of treatment/vaccine just in case this ever happened in one of these labs or am i giving the human race too much credit.
- Joined
- Oct 22, 2010
- Messages
- 21,658
very skeptical there are artificial elements in its genome. the furin cleavage site that has often been mentioned as a potential artificial insert is not what a human would put there given the choice. there are multiple lines of evidence supporting this, unfortunately i lost the link to the thread where i saw them. recapping from memory:
1. it is not a canonical site. when we insert something, we should know it works. this site works, but is unlike cleavage sites that are commonly used, all of which have been validated over decades and whose cleavage performance is stronger.
2. mutations in the site make the virus *stronger* (more infectious). a bioweapon artificially made weak...?????
none of this means the (naturally occurring) virus didn't escape from the virology lab. but it does mean that claims of genetic engineering, deliberate release, and bioweapon, should be treated very skeptically.
i read wade's long piece earlier, and he builds a strong case for lab escape, and then contradicts himself trying to make a case for genetic engineering/more. at one point he says "genetic engineering is untraceable", at another, he notes the rare, striking, *traceable* nature of the cleavage site. he's having and eating his cake on this.
e - found the thread i think:
there's another thread here which i'm less sure of, but seems to have some good info:
1. it is not a canonical site. when we insert something, we should know it works. this site works, but is unlike cleavage sites that are commonly used, all of which have been validated over decades and whose cleavage performance is stronger.
2. mutations in the site make the virus *stronger* (more infectious). a bioweapon artificially made weak...?????
none of this means the (naturally occurring) virus didn't escape from the virology lab. but it does mean that claims of genetic engineering, deliberate release, and bioweapon, should be treated very skeptically.
i read wade's long piece earlier, and he builds a strong case for lab escape, and then contradicts himself trying to make a case for genetic engineering/more. at one point he says "genetic engineering is untraceable", at another, he notes the rare, striking, *traceable* nature of the cleavage site. he's having and eating his cake on this.
e - found the thread i think:
Tweet
— Twitter API (@user) date
there's another thread here which i'm less sure of, but seems to have some good info:
Tweet
— Twitter API (@user) date
Last edited:
Stanley Road
Renaissance Man
Are people still going down this road? Ffs
Sparky Rhiwabon
New Member
- Joined
- Jul 10, 2013
- Messages
- 16,946
I feel like we’re heading for another lockdown, or at least some sort of reversal of the loosening of restrictions. Anyone else feel this way or am I just being pessimistic?
Pessimistic, the data doesn't suggest that we're heading for another lockdown.I feel like we’re heading for another lockdown, or at least some sort of reversal of the loosening of restrictions. Anyone else feel this way or am I just being pessimistic?
Sparky Rhiwabon
New Member
- Joined
- Jul 10, 2013
- Messages
- 16,946
But does the data take account of the fact that the more transmissible ”Indian Variant” will soon be rife across the UK? Can’t see how it can be isolated in small areas.Pessimistic, the data doesn't suggest that we're heading for another lockdown.
Stack
Leave Women's Football Alone!!!
Is there a jump in the numbers of new cases? Looking at the daily case numbers etc the drop from the bulk of last year is pretty massive. I know there are still people being infected and also sadly dying but its a pretty significant change. It looks to an average Joe like me that the vaccinations have helped massively. Honest question for those who understand all this more but is it likely the new Variant will see the numbers of last year or will it possibly lead to a jump in numbers but not one that will overload medical systems?But does the data take account of the fact that the more transmissible ”Indian Variant” will soon be rife across the UK? Can’t see how it can be isolated in small areas.
It currently is, Bolton's numbers dropped day on day and Blackburn's looks to have peaked. It's been noted that other areas that saw this variant had small peaks but then dropped. We had this same issue with the South African and Brazilian variant, all the data points to the vaccine having an impact on this variant too.But does the data take account of the fact that the more transmissible ”Indian Variant” will soon be rife across the UK? Can’t see how it can be isolated in small areas.
72.5% of the population have had a single jab, that will reduce hospitalisation significantly. Hospitalisation numbers are the key metric to look at now, and then have been on a downward trend since the end of Jan. I don't see any reason now why June can't happen given that I would say all will have been offered their first jab by then.
Gehrman
Phallic connoisseur, unlike shamans
- Joined
- Feb 20, 2019
- Messages
- 11,171
Gain-of-Function research is done with a vaccine in mind, but I don't believe they immidiately have a vaccine for whatever virus they are experimenting with.Too sensible for humans as a whole, but surely you would of developed some form of treatment/vaccine just in case this ever happened in one of these labs or am i giving the human race too much credit.
Gehrman
Phallic connoisseur, unlike shamans
- Joined
- Feb 20, 2019
- Messages
- 11,171
I don't think the whole notion is that it is a bioweapon, but simpy a corona virus subjected to gain-of-function research that accidently got out of the lab. It's happened many times in history where a virus has escaped a lab. It's worth noting that it's reported now that staff at the institute were hospitalized early november 2019 with symptoms similar to covid 19.very skeptical there are artificial elements in its genome. the furin cleavage site that has often been mentioned as a potential artificial insert is not what a human would put there given the choice. there are multiple lines of evidence supporting this, unfortunately i lost the link to the thread where i saw them. recapping from memory:
1. it is not a canonical site. when we insert something, we should know it works. this site works, but is unlike cleavage sites that are commonly used, all of which have been validated over decades and whose cleavage performance is stronger.
2. mutations in the site make the virus *stronger* (more infectious). a bioweapon artificially made weak...?????
none of this means the (naturally occurring) virus didn't escape from the virology lab. but it does mean that claims of genetic engineering, deliberate release, and bioweapon, should be treated very skeptically.
i read wade's long piece earlier, and he builds a strong case for lab escape, and then contradicts himself trying to make a case for genetic engineering/more. at one point he says "genetic engineering is untraceable", at another, he notes the rare, striking, *traceable* nature of the cleavage site. he's having and eating his cake on this.
e - found the thread i think:
Tweet
— Twitter API (@user) date
there's another thread here which i'm less sure of, but seems to have some good info:
Tweet
— Twitter API (@user) date
I don't think in general China's behavior has been productive in order to not seem suspicious. If you've got nothing to hide, you allow people in.
China did the opposite. Chinese authorities suppressed all records at the Wuhan Institute and closed down its database of viral genomes. China barred all international scientists from going near the caves in Yunnan; blocked the roads; confiscated samples taken by a team of scientists on a recent trip to the caves; and all research papers based on evidence from the caves must be submitted to a task force overseen by the government in Beijing "under direct orders from President Xi Jinping. When Australia lobbied world leaders in April 2020 for an inquiry into the origins of the COVID-19 pandemic, China responded with harsh trade sanctions.
Last edited:
That was part of an ongoing tiff between Australia and China and doubtful it was anything to do with a real suspicion we had.When Australia lobbied world leaders in April 2020 for an inquiry into the origins of the COVID-19 pandemic, China responded with harsh trade sanctions.
Sparky Rhiwabon
New Member
- Joined
- Jul 10, 2013
- Messages
- 16,946
That’s good then, thanksIt currently is, Bolton's numbers dropped day on day and Blackburn's looks to have peaked. It's been noted that other areas that saw this variant had small peaks but then dropped. We had this same issue with the South African and Brazilian variant, all the data points to the vaccine having an impact on this variant too.
72.5% of the population have had a single jab, that will reduce hospitalisation significantly. Hospitalisation numbers are the key metric to look at now, and then have been on a downward trend since the end of Jan. I don't see any reason now why June can't happen given that I would say all will have been offered their first jab by then.
stw2022
New Member
- Joined
- Jan 17, 2021
- Messages
- 3,687
Was ethnicity playing a part too? Bolton, Blackburn, Leicester, Bradford... these are areas with high Asian populations and we know BAME are worse affected
Yes and no. It's likely there were more seed cases - people travelling from India who had caught covid there - in those areas. The timeline suggests that the infection chains started before hotel quarantine was introduced. If you are quarantining at home, your (non-traveling) family aren't subject to quarantine - they go to work/school as normal.Was ethnicity playing a part too? Bolton, Blackburn, Leicester, Bradford... these are areas with high Asian populations and we know BAME are worse affected
Housing conditions and (very) local demographics have played the bigger role in onward transmission. In the case of Bolton, the areas where it's concentrated have the youngest demographics, and their jobs are mostly the kind that you can't do from home.
Most of the cases have happened in the uncaccinated age groups, with a high likelihood that it's spreading at school then getting the parents:
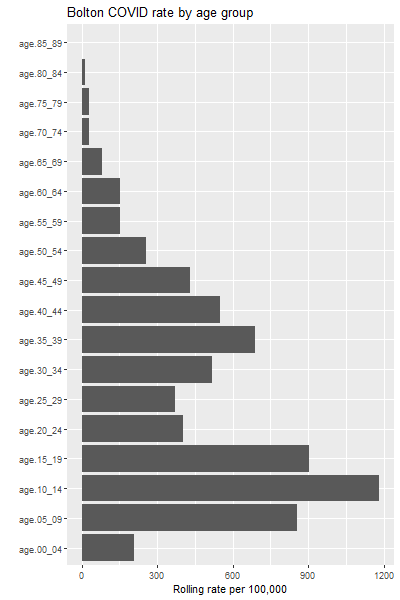
In multi-generation households (or any situation where the young have caring responsibilities, whether they live together or not) there's a high probability that it will spread into more vulnerable age/risk groups. The unvaccinated, partly vaccinated are obviously then at most risk - but unlucky vaccinated ones are at risk as well (vaccines aren't 100% effective, though the covid ones get close) - which is why the hospital figures are rising now.
Massive Spanner
Give Mason Mount a chance!
Oh @Pogue Mahone won't like that graph.